Internal Carotid Artery Bifurcation Aneurysm



This is a preview. Check to see if you have access to the full video. Check access
Clip Ligation of an ICA Bifurcation Aneurysm
Aneurysms at the bifurcation of the internal carotid artery (ICA) are uncommon lesions, accounting for approximately 5-10% of intracranial aneurysms. They frequently occur in conjunction with other aneurysms on the ipsilateral ICA, and appear to be more prevalent among the pediatric population. The hemodynamic stress at the ICA bifurcation, like the one at the basilar bifurcation, leads to aneurysm formation.
The middle cerebral artery (MCA) and ICA are the vessels most likely to harbor mirror aneurysms. These aneurysms occur in 5-10% of patients with single aneurysms and in 36% of patients with multiple aneurysms. Notably, mirror aneurysms are more likely to rupture and tend to rupture earlier in life.
Rupture of an ICA bifurcation aneurysm causes subarachnoid hemorrhage (SAH) and may even cause intracerebral hemorrhage (ICH) in the inferior frontal lobe, basal ganglia, or medial temporal lobe. Most ICA bifurcation aneurysms point superiorly and slightly posteriorly.
Preservation of the medial and posterior perforators arising from the medial borders of the A1, ICA bifurcation, anterior choroidal artery, recurrent artery of Heubner, and M1 segments is imperative during dissection of the aneurysm neck and clip deployment.

Atlas Choice Tapered Pattie Collection
Low-profile for maximal visualization and protection
Tapered shape designed for retractorless surgery
Unparalleled flexibility and non-stick features
Indications for Surgery
The ICA aneurysms carry a fairly low annual rupture risk of ~1% until they grow larger than 25 mm, at which point their annual rupture risk increases to 10%.
Numerous factors affect the need for treatment, including the age and general health of the patient, a first-degree relative with a history of SAH, and the specific characteristics of the aneurysm such as demonstrated growth, abnormal aneurysm morphology, and the presence of a blister on the dome. Aneurysms in this location are almost never symptomatic secondary to their mass effect.
With an appropriate neck-to-dome ratio, these aneurysms may be treated with endovascular therapy alone. If the proximal segment of the parent A1 or M1 is incorporated into the aneurysm neck, balloon-assisted or stent coiling are possible treatment options. Flow-diverters are not commonly used for ICA bifurcation aneurysms at this time, but this technology is rapidly expanding the indications for endovascular intervention.
Preoperative Considerations
In the absence of SAH, the ICH caused by ICA bifurcation aneurysms can mimic hypertensive basal ganglia hemorrhage. Calcified aneurysms are more suitable for endovascular intervention but the risk of coil compaction is significant due to the direct hemodynamic stress of the afferent high flow ICA.
Preoperative imaging including CT angiography frequently demonstrates the extension of the aneurysm neck more on the A1 rather than M1. This anatomy is important for surgical planning and trajectory of clip application. The presence of a functional anterior communicating artery (ACoA) indicates the ischemic tolerance and safety of proximal A1 ligation in the event of intraoperative rupture.
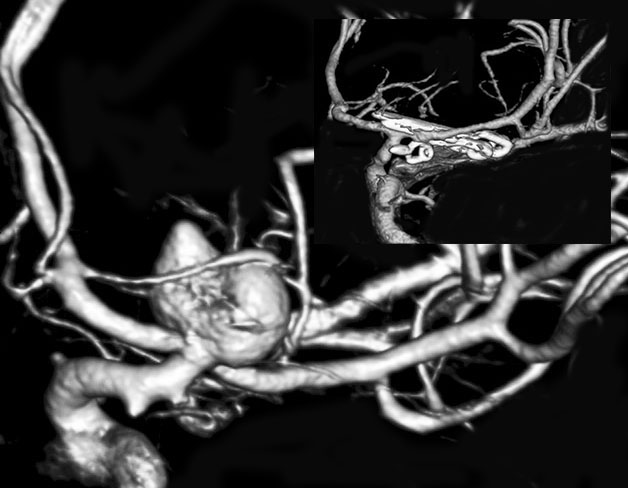
Figure 1: A classic ICA bifurcation aneurysm is demonstrated. Note the perforating vessel draping over the dome. Clip exclusion was accomplished via tandem clipping (inset). The small anterior choroidal aneurysm was also clipped in this patient.
Operative Anatomy
Aneurysms of the ICA bifurcation have been compared with basilar bifurcation aneurysms in the basic details of their anatomy. They arise from the bifurcation of a major vessel, potentially incorporating a variable extent of each afferent and efferent branch into their aneurysm neck, with numerous perforators located at the medial or posterior base of the aneurysm.

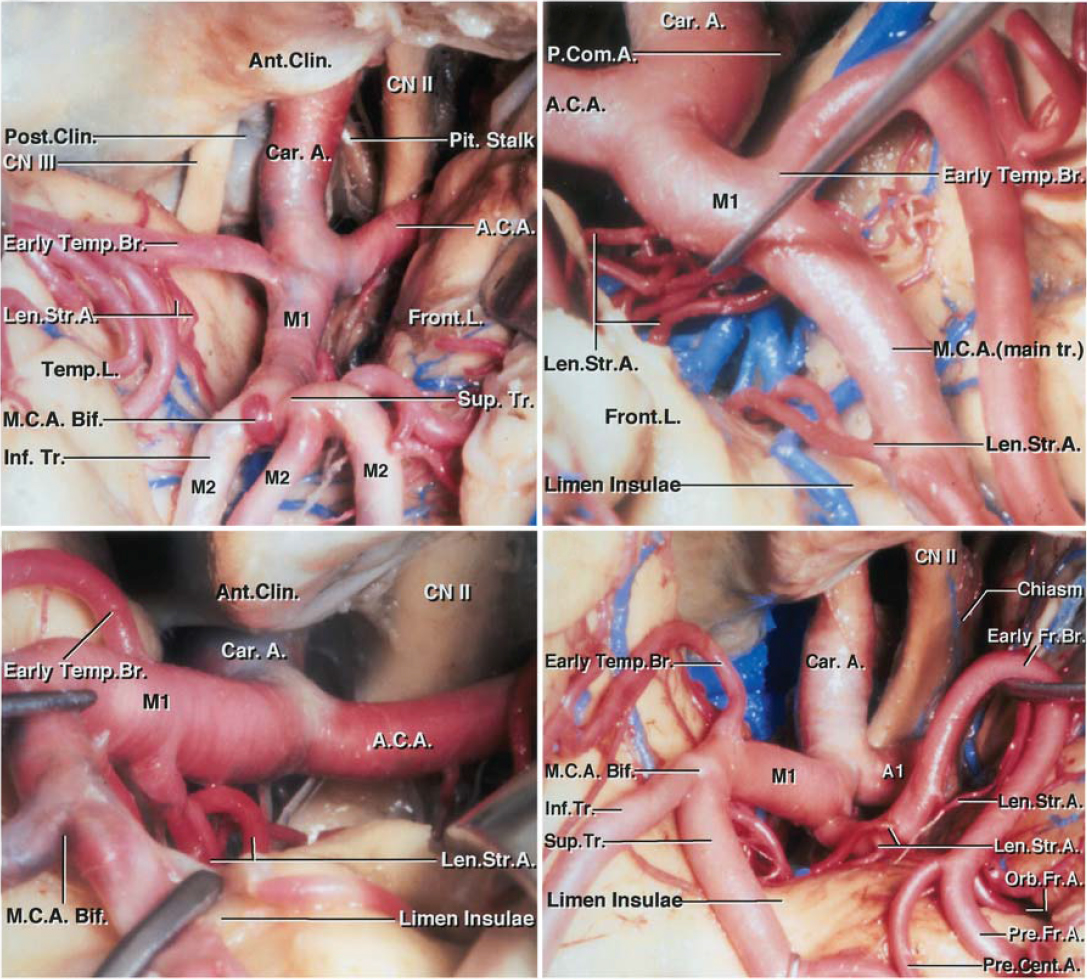
Figure 2: The right supraclinoid ICA bifurcates into the M1 branch of the MCA and the A1 branch of the anterior cerebral artery (ACA,) within the proximal sphenoidal segment of the Sylvian fissure. The M1 courses posterolaterally further into the fissure, while the A1 turns medially to cross over the optic nerve and chiasm. Note the perforating vessels arising from the proximal A1 and M1 branches.
Aneurysms of the ICA bifurcation usually arise from the posterior aspect of the ICA and are often eccentric toward the A1. The artery is normally oriented superiorly and posteriorly, thus its aneurysms also project in these directions. Two groups of lenticulostriate arteries (LSAs) arise near the ICA bifurcation: medial and lateral. The lateral LSAs arise from the M1 segment, and the medial LSAs arise from the A1 segment. The bifurcation proper is often devoid of these perforators that are often adherent to the aneurysm dome and complicate clip application.
The recurrent artery of Heubner is the most medial and anterior of the medial LSAs, often arising laterally from the ACA at the A1–A2 junction and travelling parallel to A1 posteriorly. The surgeon should look for this recurrent artery, which may be the first vessel encountered when he or she is dissecting subfrontally along the superior aspect of the optic nerve.
The most superior nonterminal branch of the supraclinoid ICA is the anterior choroidal artery. In patients with posteriorly and medially projecting aneurysms, the dome may become intimately involved with this artery or its perforating branches. Temporary occlusion of the ICA, mobilization of the dome, and sharp dissection of the artery are needed to avoid its sacrifice.
The medial and lateral LSAs pose the greatest challenge to the operator given their location posterior and medial to the aneurysm dome and within the operative blind spot. These vital perforators extend superiorly into the anterior perforated substance, optic apparatus, and medial temporal lobe. They can be microscopic and intimately adherent to the posterior and medial aneurysm neck and/or dome. Their manipulation can lead to vasospasm or even their dissection. Liberal use of papaverine is advised.
Click here to view the interactive module and related content for this image.
Figure 3: The anatomy of ICA bifurcation and relevant lenticulostriate arteries (Len. St. A.) is shown. Wide Sylvian fissure dissection provides the most effective corridor to the bifurcation.
MICROSURGICAL CLIP LIGATION OF ICA BIFURCATION ANEURYSMS
The extended pterional craniotomy is typically employed for clip ligation of ICA aneurysms. The patient’s head is rotated 30 degrees and the malar eminence is the highest point in the operative field. This head posture minimizes intrusion of the temporal lobe by its collapse on the transsylvian corridor.
The craniotomy extends just above the superior temporal line. Resection of the lateral sphenoid wing expands the operative space toward the ICA bifurcation.
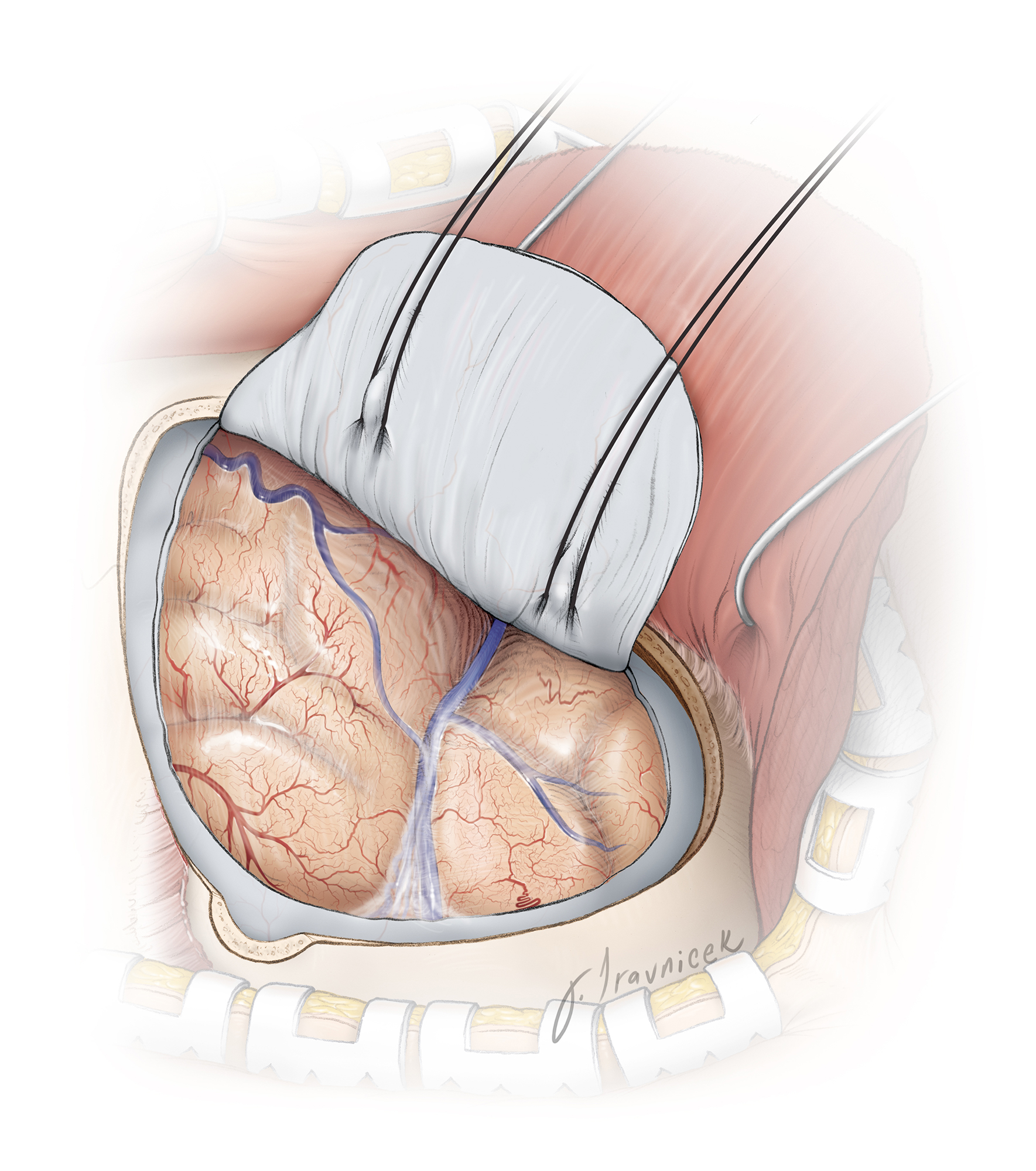
Figure 4: The breadth of the pterional craniotomy for this aneurysm type is illustrated. Significant frontal extension of the craniotomy is typically unnecessary. The lateral sphenoid wing is resected to the level of the superior orbital fissure.
INTRADURAL PROCEDURE
Initial Exposure
Similar to MCA bifurcation aneurysms that may be exposed from distal-to-proximal or proximal-to-distal, there are also two strategies for subarachnoid dissection to expose ICA bifurcation aneurysms.
Technique 1: The Inside-Out Technique
The first technique is referred to as the inside-out technique, whereby the parasellar and opticocarotid cisterns are split first, and then the Sylvian fissure is dissected from proximal to distal, while following the course of the ICA, to expose the carotid bifurcation. Gentle elevation of the posterior basal frontal lobe expands the desired operative pathway toward the bifurcation.
In my experience, proximal-to-distal dissection of the fissure is technically awkward and exerts undue retraction on the basal frontal lobe.
Technique 2: The Outside-In Technique
The second technique begins with a distal Sylvian fissure split, with pursuit of the anterior and inferior aspects of M1 to expose the carotid bifurcation through the horizontal limb of the fissure. The supraclinoid ICA is identified and dissection proceeds along the ICA to the bifurcation. The proximal M1 and A1 segments are exposed. The A1 segment must be thoroughly unveiled because ICA bifurcation aneurysms are often eccentric toward the A1; this efferent vessel is intimately involved with the neck.
I routinely use the outside-in technique, especially for ruptured aneurysms, to minimize the degree of frontal lobe retraction on a swollen post-SAH brain. Both techniques require identification of the proximal ICA distal to the anterior choroidal artery for placement of a temporary clip should this become necessary. This maneuver often requires division of a small bridging vein found along the anterior Sylvian fissure and lateral to the optic nerve.

Figure 5: The Sylvian fissure dissection is carried medially and posteriorly into the horizontal segment of the fissure to expose the supraclinoid ICA and bifurcation. This approach provides early proximal control and brain relaxation via cerebrospinal fluid egress through the corresponding cisterns. The anterior choroidal artery along the posterior wall of the carotid is identified and protected during temporary clip deployment.
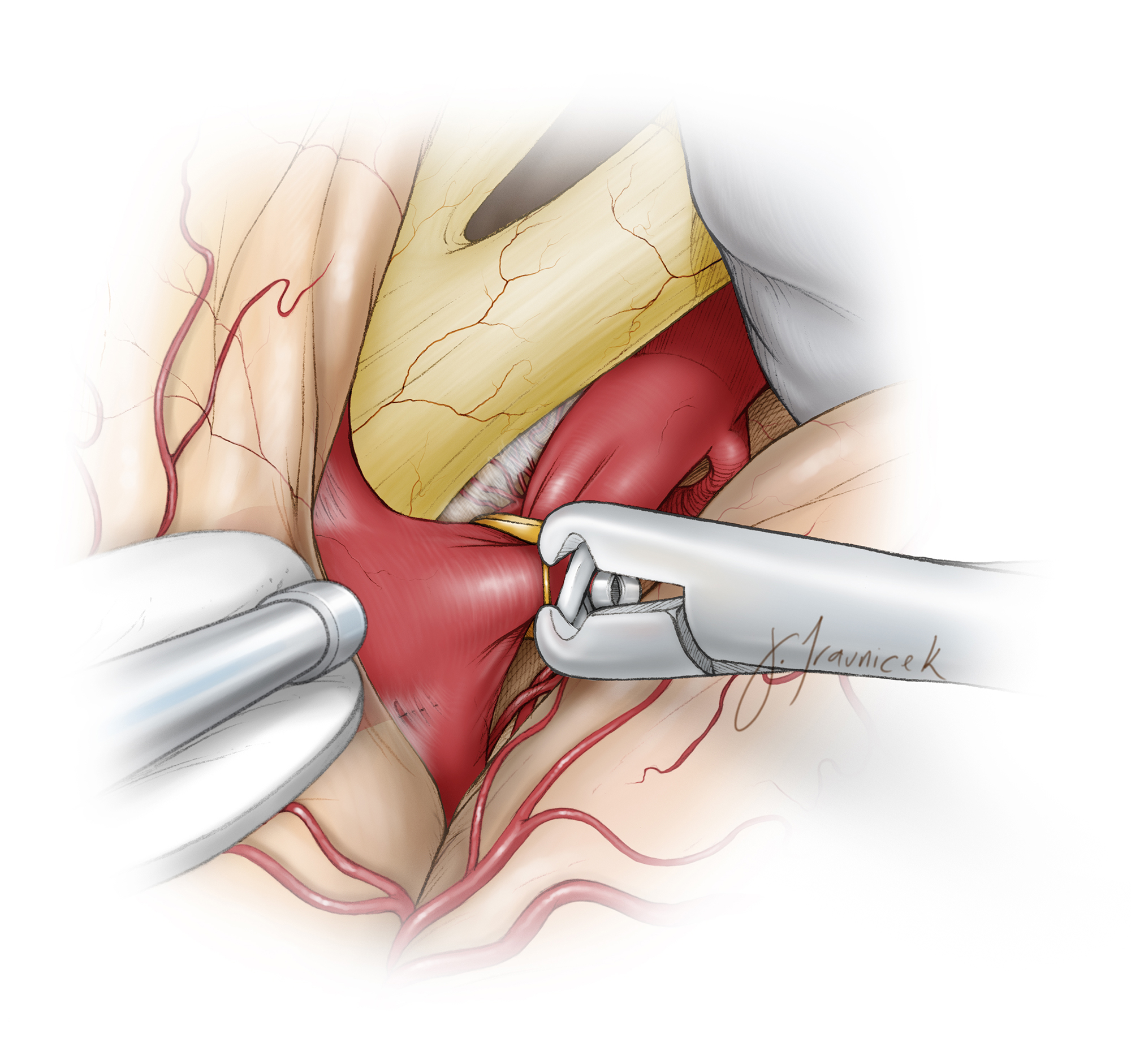
Figure 6: Gentle mobilization of the medial posterior basal frontal lobe is necessary to avoid premature intraoperative rupture of the aneurysm sac that is embedded in this portion of the lobe. The location of the temporary clip distal to the anterior choroidal artery is shown. I use temporary clipping liberally so that I can mobilize the neck laterally and dissect the A1 and M1 perforating vessels away from the medial wall of the aneurysm neck.
Aneurysm Dissection
Once proximal control has been secured, the final dissection of the aneurysm begins at the lateral neck between the aneurysm and the M1, rather than at the A1.
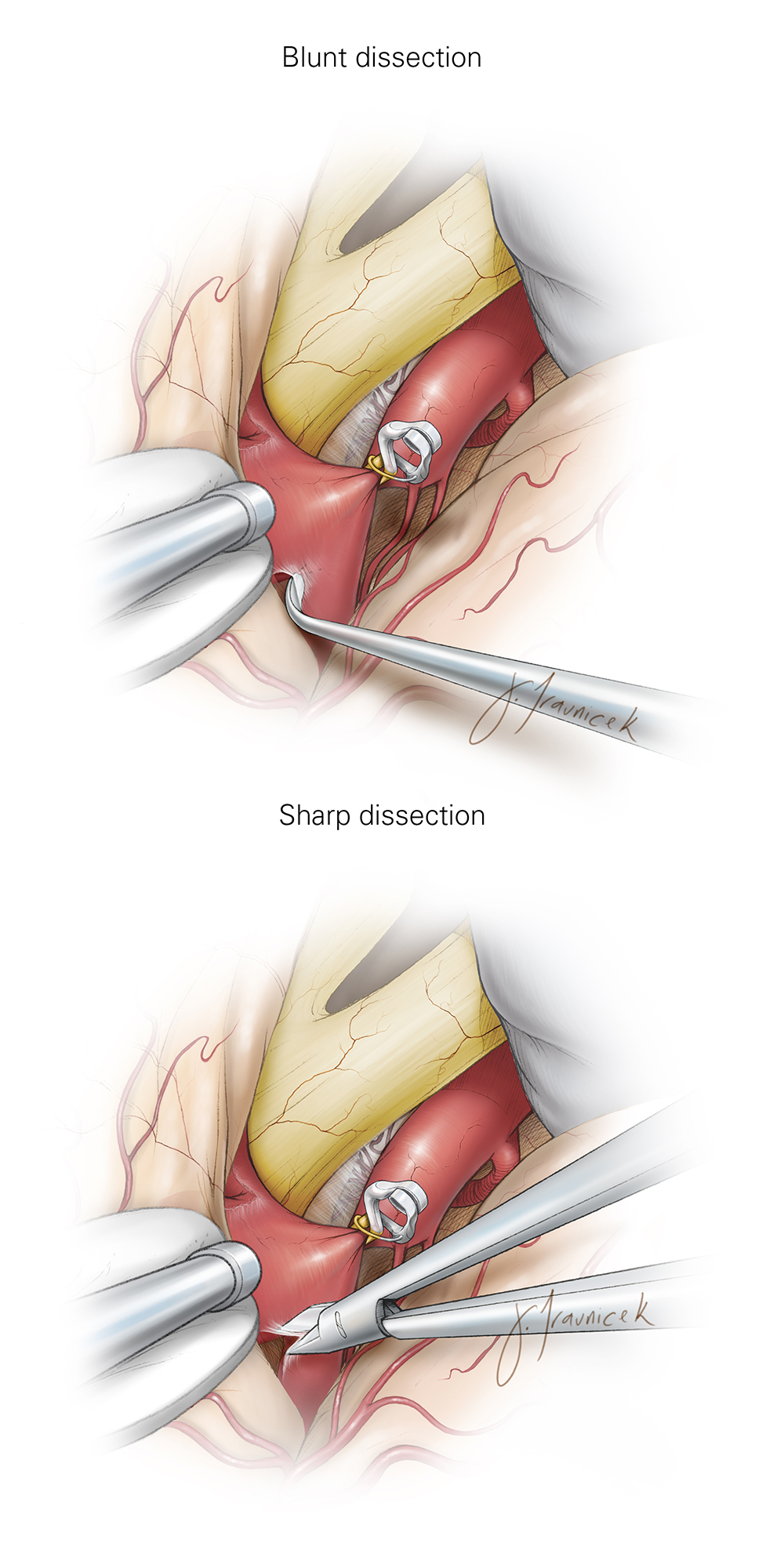
Figure 7: The order of dissection at the M1 before A1 is illustrated. The blunt technique (top image) is generally avoided and sharp dissection is used (bottom image). This order of dissection is important because isolation of the medial neck between the A1 and the aneurysm is often more challenging. In addition, if an intraoperative rupture occurs after the isolation of M1, a temporary clip may be placed to incorporate the aneurysm and the proximal A1. This maneuver will maintain anterograde irrigation of the M1 and retrograde irrigation of the A1 via the anterior communicating artery complex. The temporary clip may be exchanged with a permanent clip if the neck tear is not amenable to the cotton-clipping technique (please see Figure 18 below.)
I continue dissection medially on the neck toward the A1. For both sides of the neck, sharp/blunt dissection under high magnification is the preferred method for developing the plane between the M1/A1 and the neck. All the perforators have to be spared.

Figure 8: For larger or more broad-based aneurysms, I need a wider viewing space parallel to the medial wall of the neck to dissect the perforators. To do so, I split the fissure along the proximal M1 more thoroughly to expand the working angle behind the neck.
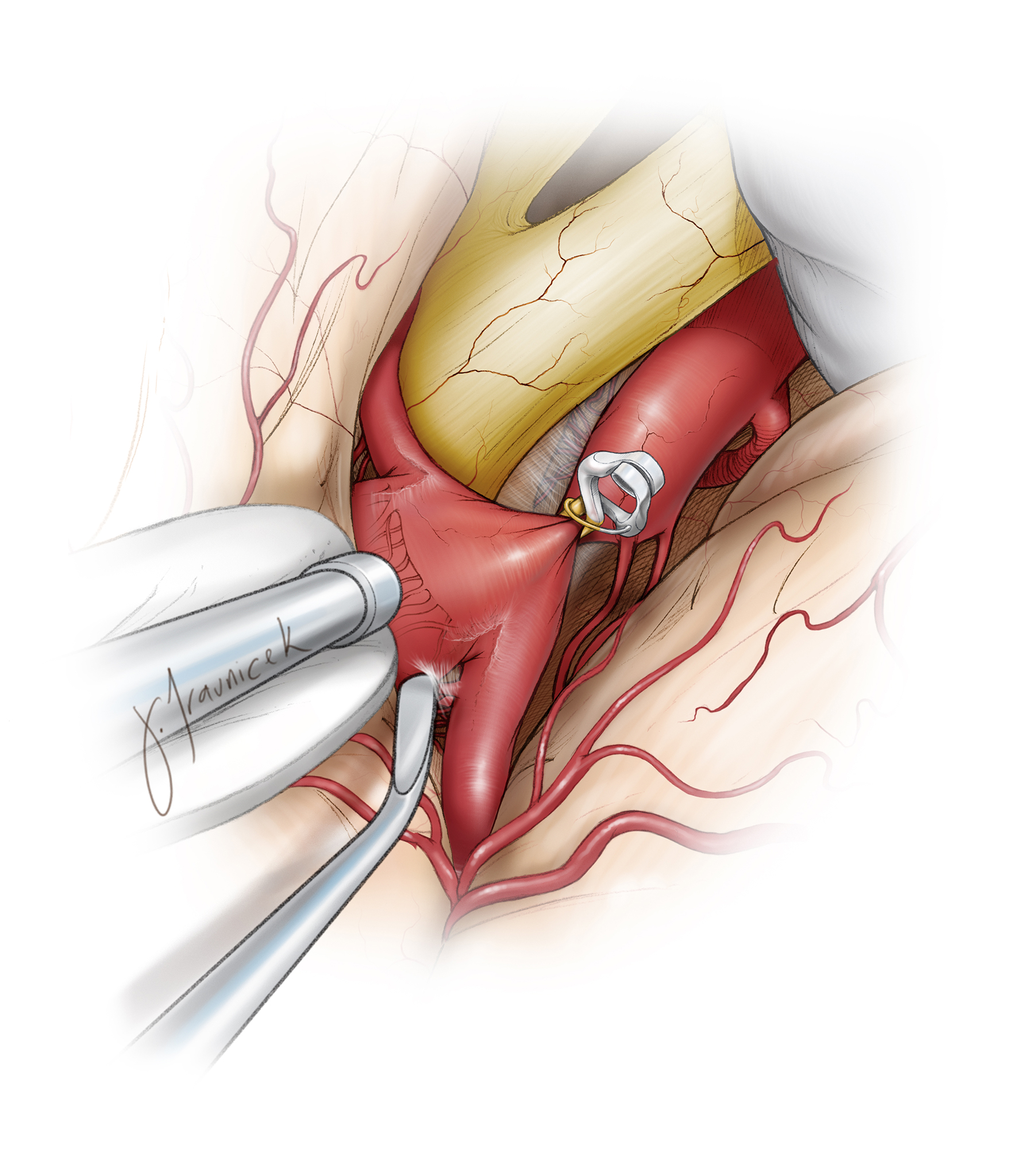
Figure 9: The posterior aspect of the neck can obscure the adherent perforators and the anterior choroidal and Huebner arteries. More thorough mobilization of the sac is often needed using temporary clip ligation of the proximal ICA. The surgeon should remain diligent and persistent, fully exploring this area of the neck to confirm that it has been cleared of all perforating vessels. Blind passage of the blades of the permanent clip should be avoided.
Finally, the distal neck along the A1 is isolated while the surgeon works lateral and medial to the neck. I ensure clear visualization of the medial neck from its base along the M1 all the way to the A1 so that a clear path for the blades is secured.

Figure 10: Small Gelfoam pledgets may be inserted to keep the perforating vessels away from the neck for broad-based aneurysms. During passage of the final permanent clip blades, the tips of the blades push these pledgets forward; however, the perforating vessels remain protected. Please see Figure 12 below for more details.
Clip Application
The optimal clip construct depends on the projection of the aneurysm dome. For the typical superiorly and posteriorly projecting aneurysms, a straight or slightly angled clip is effective. The angled clip provides better visualization of the blades during their insertion.

Figure 11: A slightly angled clip is used to collapse the aneurysm neck. Once the blades are in place around the neck, the blades are gently approximated while any stenosis or inadvertent kink in the MCA origin is avoided. The exact location of the clip blades along the neck often needs to be gently and slightly adjusted to avoid any neck remnant and compromise of the M1’s and A1’s origins.
One of the minimally viewable spots during clip application is the proximal A1, especially if the anatomy of the aneurysm neck and bifurcation positions this vessel coursing away from the surgeon’s line of sight. In these instances, the final moments in the slow gradual closure of the clip blades barely reveals the origin of A1, allowing an opportunity for minor adjustments in clip position. Clip repositioning may be necessary for a desirable construct.
If the neck is asymmetrically shared by the proximal M1, a straight clip is more appropriate. However, if the neck is predominantly on the proximal A1, a slightly angled clip is potentially more desirable so that the neck is closed parallel to the A1 parent vessel, avoiding an accordion effect that can collapse the inlets of the perforating vessels.

Figure 12: As mentioned above, very small pieces of Gelfoam may be inserted on the medial surface of the neck to keep the numerous perforating vessels away from the pathway of the medial blade. As the medial clip blade slides around the neck, these Gelfoam pledgets are pushed forward and the perforators are protected.

Figure 13: After final application of the clip, fluorescence videoangiogram confirms complete aneurysm occlusion and patency of the parent and perforating vessels. The perforators may not be easily visible using fluorescence. Next, I perforate the dome with a needle to confirm its complete exclusion from the circulation. Suction can evacuate the intrasaccular blood and collapse the sac (inset image).
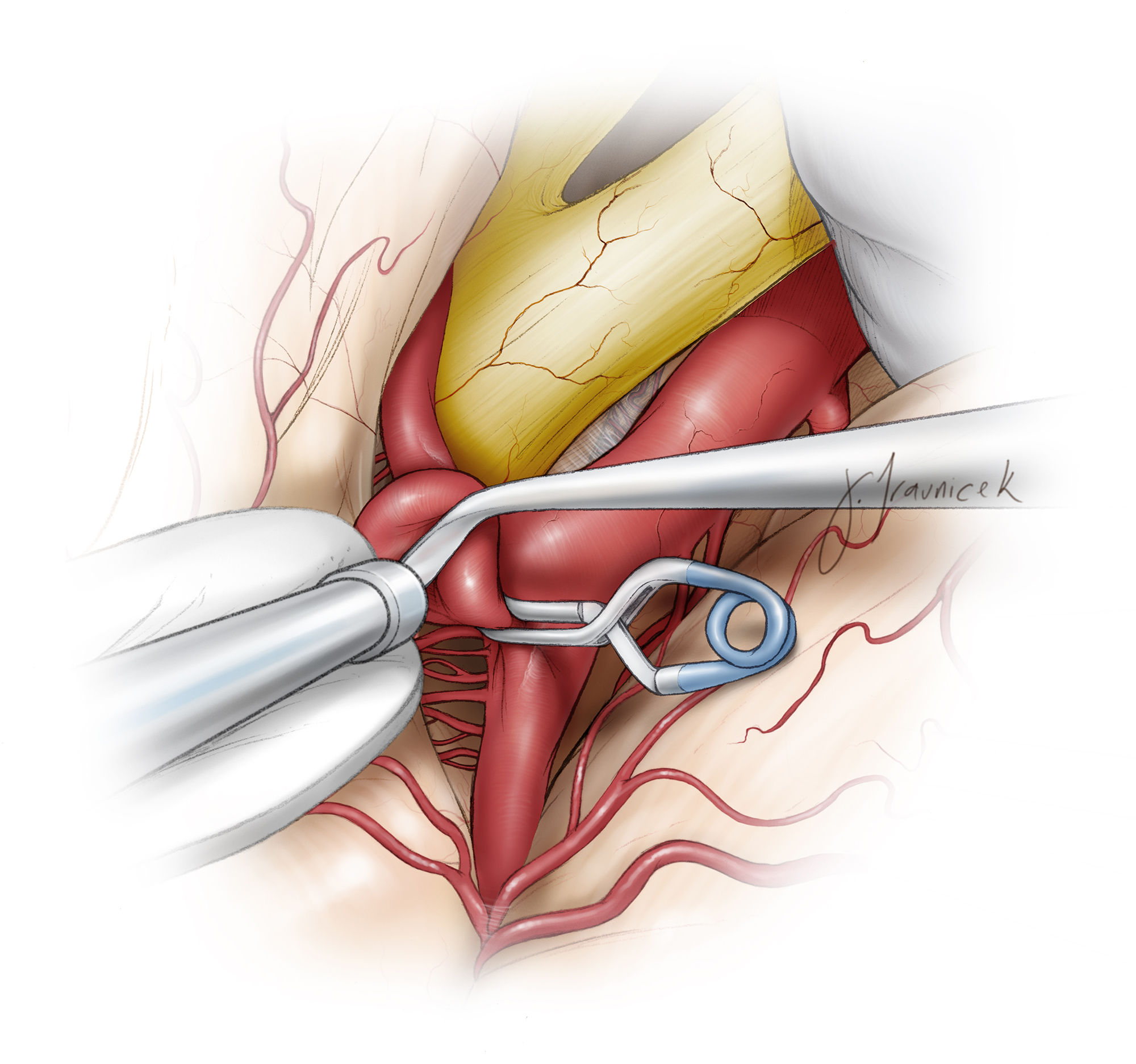
Figure 14: A circumferential dissection around the collapsed sac is mandatory to confirm the patency of the perforators. Neck remnant may require clip repositioning after reapplication of a temporary clip on the ICA.

Figure 15: A small right-sided ICA bifurcation aneurysm is demonstrated (upper image). Note the perforator behind the aneurysm neck (lower left image). This aneurysm was clipped using a small straight clip (lower right image).
Small ICA Bifurcation Aneurysm

Figure 16: A large right-sided aneurysm was clip ligated using a straight clip. The posterior pole of the sac (left upper image) was inspected under temporary ICA occlusion before clip deployment (right upper image). Atherosclerotic aneurysms may demand tandem clipping (lower image-an anterior choroidal aneurysm was also clipped in this patient). Note the dissection of the M1 perforators (lower image-right upper inset).
Large ICA Bifurcation Aneurysm

Figure 17: A patient with a giant calcified ICA bifurcation aneurysm (upper image) underwent high-flow radial artery (ECA-ICA) (middle image) bypass followed by definitive proximal occlusion of the ICA (lower image) distal to the anterior choroidal artery.
Giant Calcified and Partially Thrombotic ICA Bifurcation Aneurysm
Aneurysmal Variations
Numerous variations are possible for an ICA bifurcation aneurysm, and knowledge of these variations is important during operative planning.

Figure 18: An ICA bifurcation aneurysm was clipped using a simple straight clip (left image) or an angled clip (right image). The angled clip may avoid the MCA branch, ensuring that the hinge of the clip does not kink its lumen.
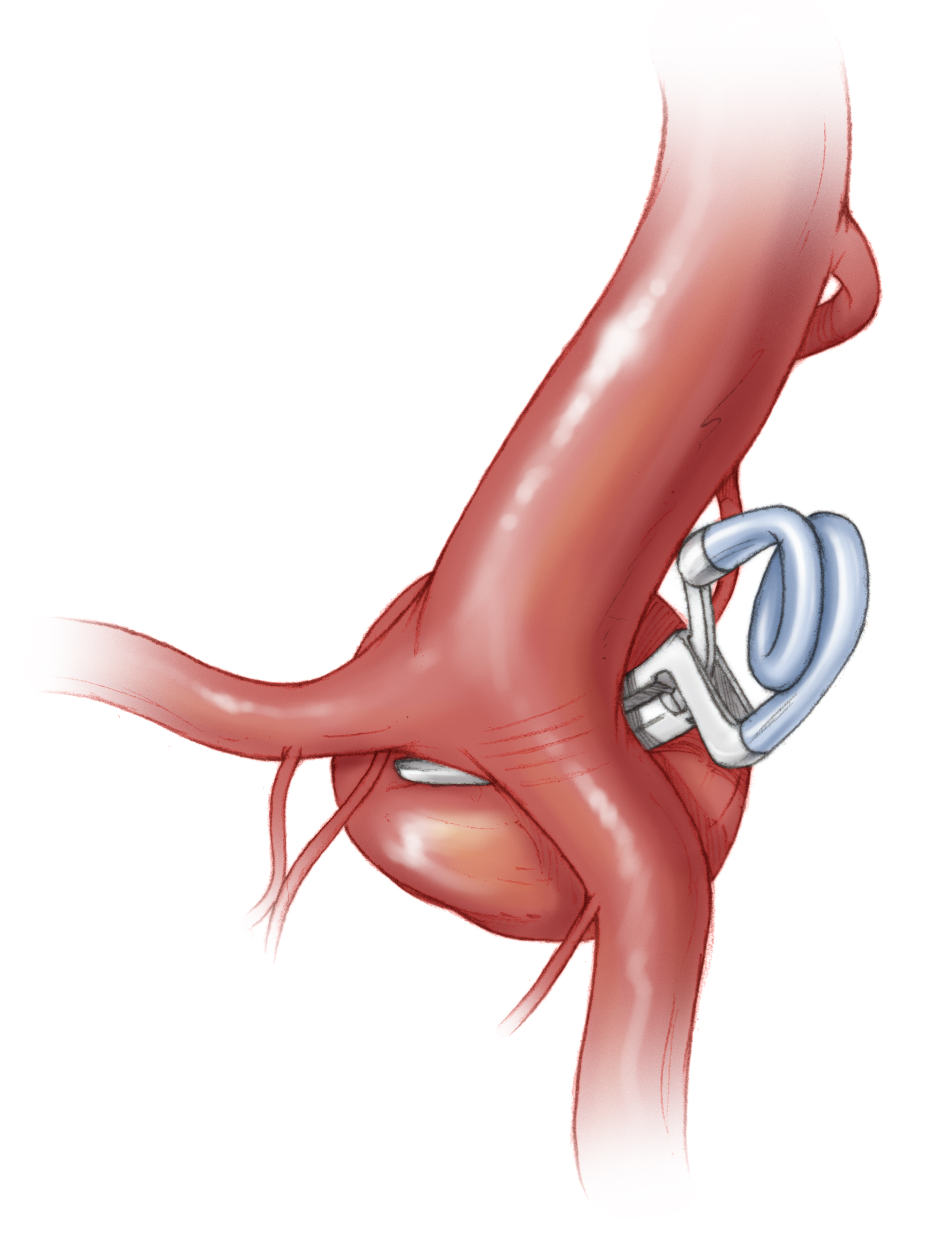
Figure 19: Medially-projecting ICA bifurcation aneurysms may be clip ligated using a curved clip. The curved clip nicely contours the bifurcation, allowing easy visualization and limited interaction with the perforating vessels. The anterior choroidal artery may need to be dissected away from the neck.

Figure 20: Broad-based medially projecting ICA bifurcation aneurysms may also be occluded via an angled fenestrated clip. The fenestration encases the MCA or any of its perforating arteries.
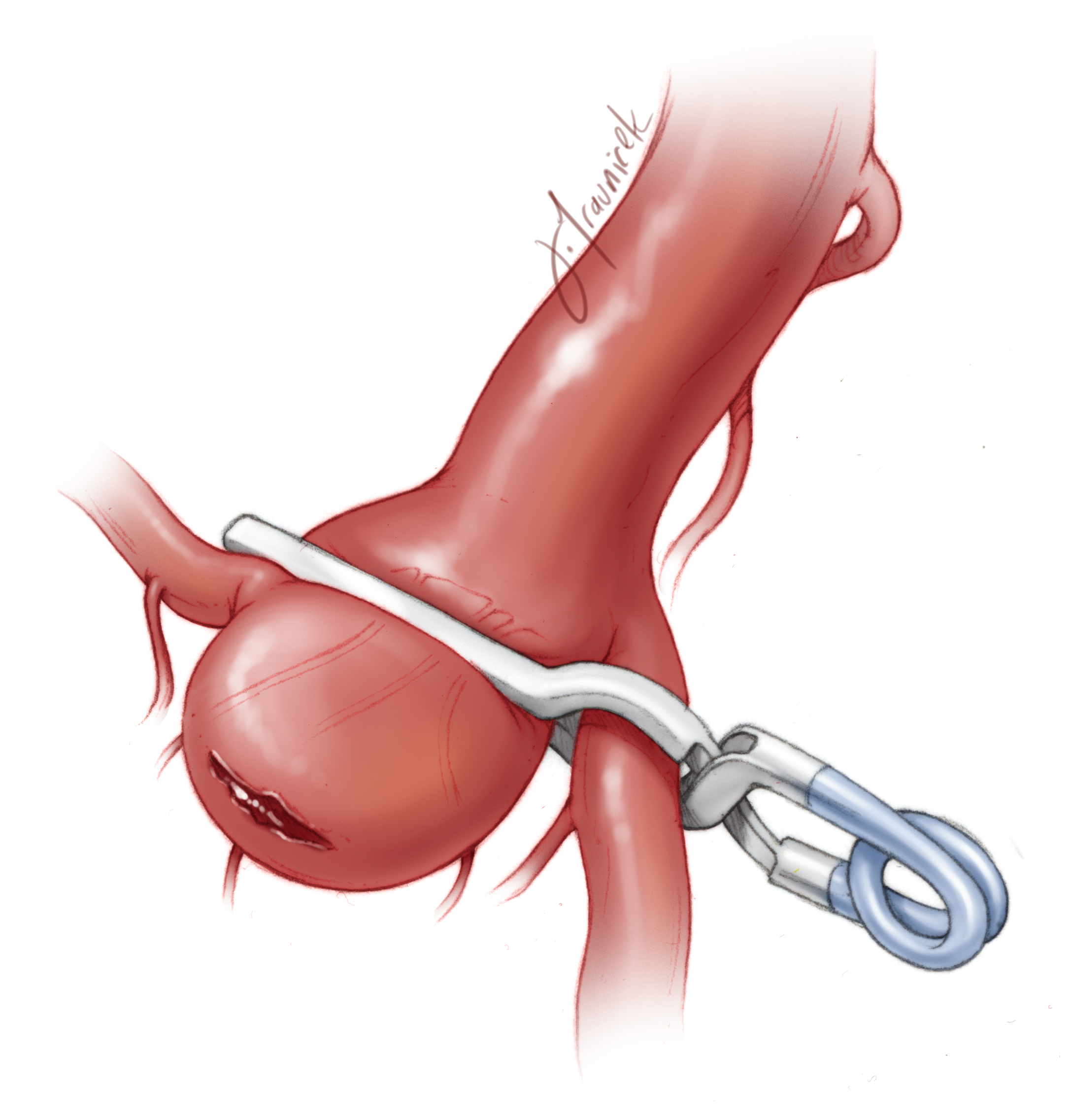
Figure 21: If an intraoperative rupture occurs after the isolation of M1, a temporary clip may be placed to incorporate the aneurysm and the proximal A1. This maneuver will maintain anterograde irrigation of the M1 and retrograde irrigation of the A1 via the anterior communicating artery complex. The temporary clip may be exchanged with a permanent clip if the neck tear is not amenable to the cotton-clipping technique.
Postoperative Considerations
Perforator injury often causes thalamic, hypothalamic, striatal, and capsular infarcts, resulting in contralateral hemiplegia and behavior changes. These changes often resolve within months, depending on the exact location and size of the infarct.
I have occasionally witnessed these infarcts in the absence of any perforator compromise during final intraoperative inspection. The closure of the aneurysm neck may lead to regional hemodynamic changes that compromise the quality, but not the quantity, of flow in these vessels.
Injury to the anterior choroidal artery of its perforating vessels often results in contralateral hemiplegia from involvement of the posterior limb of the internal capsule, hemisensory loss from involvement of the ventral posterolateral nucleus of the thalamus, and less frequently, homonymous hemianopsia from involvement of the lateral geniculate body or the geniculocalcarine tract.
Injury to the recurrent artery of Heubner often leads to a stroke in the ipsilateral head of the caudate, anterior limb of the internal capsule, and anterior third of the putamen. These infarcts often cause contralateral hemiplegia, predominantly affecting the patient’s face and upper extremities. Dominant infarcts affect speech.
Pearls and Pitfalls
- The most common source of morbidity is any compromise of the M1, A1, and anterior choroidal perforating arteries.
- Aneurysm decompression and sharp perforator dissection are important maneuvers in microsurgery of ICA bifurcation aneurysms.
Contributors: Christopher Kellner, MD and Jeremiah Johnson, MD
References
Batjer HH. Aneurysms of internal carotid bifurcation, in Samson DM (ed): Intracranial Aneurysm Surgery: Techniques. Mount Kisco, NY: Future Publishing, 1990.
Related Materials
Available Through the Atlas
-

Treatment of intracavernous and giant carotid aneurysms by combin...
-
Pediatric cerebral aneurysms
-
Microsurgical anatomy of the early branches of the middle cerebra...
-
Surgical anatomy of the proximal anterior cerebral artery
-
The hemodynamic importance of the geometry of bifurcations in the...
-
Blood blister-like aneurysms of the internal carotid artery trunk...
-
Bifurcation geometry and the presence of cerebral artery aneurysm...
-
Hemodynamic differences between unruptured and ruptured intracran...
-
Confirmation of blood flow in perforating arteries using fluoresc...
-
Proximal carotid ligation for internal carotid aneurysms. A long...
Unavailable Through the Atlas
-
Intracranial aneurysms in the pediatric population: Case series a...
-

Aneurysms
-
Complex intracranial aneurysms: Combined operative and endovascul...
-
Intracranial aneurysms and subarachnoid hemorrhage in children an...
-
Microneurosurgical management of proximal middle cerebral artery...
-
Pediatric intracranial aneurysms - Clinical characteristics and o...
-
Microsurigical anatomy of the proximal middle cerebral artery and...
-
In vivo study of flow pattern at human carotid bifurcation with r...
-
Surgical management of aneurysms of the bifurcation of the intern...
-
Treatment of giant and large internal carotid artery aneurysms wi...
-
Characteristics of aneurysms of the internal carotid artery bifur...
-
The perforating branches of the internal carotid artery: The micr...
-
Microneurosurgical management of internal carotid artery bifurcat...
Please login to post a comment.