Hypothalamic Hamartoma



This is a preview. Check to see if you have access to the full video. Check access
Resection of a Hypothalamic Hamartoma via the Supraorbital Craniotomy
A hamartoma is a benign, noncancerous growth consisting of an abnormal mixture of native tissue. Although this tumor-like lesion resembles a neoplasm, it does not exhibit neoplastic tendencies such as accelerated growth, local invasion of surrounding tissues, or metastatic spread.
Hypothalamic hamartomas are exceedingly rare developmental anomalies classically associated with endocrine abnormalities and epilepsy. They consist of a mixture of hyperactive neuronal and glial cells arising from the floor of the third ventricle.
Their true incidence is unknown, but is estimated at one in 50,000 to one in one million. Although classically associated with gelastic seizures, hypothalamic hamartomas are also responsible for several other types of more debilitating medically refractory seizures. Endocrine abnormalities, including central precocious puberty, have also been implicated.
Behavioral, psychiatric, and cognitive impairments appear to have a higher incidence in this patient population as well. In their extreme form, hypothalamic hamartomas lead to disabling epilepsy, severe cognitive deficits, and developmental delay in early childhood.

ATLAS Choice Bipolar Forceps
Designed for your every surgical maneuver
Five tip sizes for brain and spine procedures
Unparalleled non-stick and low-profile features
Diagnosis
A patient with a hypothalamic hamartoma may present with signs and symptoms of precocious puberty and/or seizures. Gelastic seizures, spells of uncontrollable laughter, were first reported in the 19th century and are considered a hallmark clinical finding.
The laughing events are typically first noted in early childhood, and may progress to include other seizure types, including generalized tonic-clonic seizures, partial complex seizures, drop attacks, and atypical absences. As stated before, behavioral, psychiatric, and cognitive changes may also be present. Additionally, gelastic seizures have been reported in the absence of any obvious imaging finding and thus cannot be considered a pathognomonic feature.
Depending on the individual patient’s presentation, the diagnostic workup often includes a full spectrum of labs, electroencephalogram (EEG), and magnetic resonance (MR) imaging.
Evaluation
Diagnostic workup of patients with seizure disorders includes MR imaging. Hypothalamic hamartomas typically demonstrate increased signal on T2-weighted images relative to the brain. MR spectroscopy studies have consistently shown decreased neuronal density and increased gliosis.
Several studies have evaluated the EEG findings in these patients. Scalp EEG often fails to show ictal or interictal abnormalities if the seizure semiology is confined to gelastic seizures alone. As this disease progresses and secondarily generalized seizures appear, scalp EEG reveals abnormal findings. Multiple seizure types lead to frontal or temporal multifocal activities. Cortical resection has been ineffective at controlling seizures. Depth electrode evaluation has confirmed the hypothalamic hamartoma as the ictogenic source.
There are two subtypes of hypothalamic hamartomas, differing on the basis of their anatomic relationship to the normal hypothalamic tissue. Sessile hypothalamic hamartomas harbor a broad base with local invasion and displacement of the adjacent surrounding hypothalamic tissue. Pedunculated hypothalamic hamartomas, on the other hand, are suspended by a stalk-like process from the floor of the third ventricle. Sessile hamartomas are more likely to cause epilepsy, whereas pedunculated lesions are associated with endocrine abnormalities.

Figure 1: A 23-year-old man presented with intractable multifocal epilepsy associated with gelastic seizures. MR imaging revealed a T2 hyperintense, nonenhancing mass along the anterior floor of the third ventricle consistent with a sessile hypothalamic hamartoma.
Indications for Surgery
Evidence-based management algorithms are difficult to establish for such rare lesions. In general, surgical indications include seizures intractable to maximal medical therapy. Precocious puberty is another indication for intervention that leads to regression of preoperative symptoms and signs.
Several studies have confirmed the primary and secondary epileptogenicity of hypothalamic hamartomas. Thus, patients with an uncontrollable seizure disorder who have a known hypothalamic hamartoma are suitable candidates for operative intervention.
Preoperative Considerations
Various surgical approaches to the anterior third ventricle have been described in the literature, including standard pterional, transcallosal, endoscopic transventricular, endoscopic endonasal, and subfrontal translamina terminalis. A standard pterional approach is familiar to neurosurgeons and offers a relatively direct route to the lesion. However, visualization of the anterior third ventricle is limited by the critical overlying neurovascular structures with this approach. Thus, significant retraction and manipulation of the normal anatomy may be needed to conduct the resection.
A transcallosal approach provides a direct vertical route to the anterior third ventricle and clear visualization of the intraventricular aspects of the lesion. Limitations of this approach include the risks of memory disturbance from forniceal manipulation.
Endoscopic endonasal access has great potential for providing a minimally disruptive option to this lesion, but the experience for the use of this route is limited.
I favor the subfrontal translamina terminalis approach through a supraorbital craniotomy. Some degree of frontal lobe retraction is necessary to reach the lesion via a superior-to-inferior operative trajectory toward the floor of the third ventricle. Additionally, a contralateral subfrontal pathway creates a more direct surgical corridor to the lateral pole of the mass.
Radiosurgery is a viable consideration for the treatment of hypothalamic hamartomas. The potential limitations of radiotherapy include a delayed response to treatment and the risk of radiation injury to the hypothalamus and optic apparatus; these factors limit radiotherapeutic dosing and, in turn, can limit treatment effectiveness.
Operative Anatomy
Knowledge of the anatomy of the lamina terminalis and the floor of the third ventricle is essential for safe and effective removal of these lesions. Please refer to the Subfrontal Translamina Terminalis Approach chapter for further details.
Embryologically, lamina terminalis represents the most rostral end of the developing neural tube. This structure represents the widest region of the third ventricle and attaches at an acute angle to the midportion of the optic chiasm, forming the optic recess posteriorly. Anterior to the lamina is its cistern, part of the suprachiasmatic cistern which contains the A1 segments of the anterior cerebral arteries, anterior communicating artery, recurrent arteries of Heubner, frontoorbital arteries, hypothalamic perforators, proximal A2 segments, anterior communicating vein, and the anterior cerebral vein.

Figure 2: Note the anatomy of the lamina terminalis in relation to the anterior cerebral arteries and their septal and hypothalamic perforating vessels (left image). The boundaries of the lamina terminalis are marked with yellow arrows. Upon opening the lamina terminalis, the floor of the third ventricle is evident (right image). A relatively acute superior-to-inferior working angle is necessary to reach the floor via the subfrontal trajectory (images courtesy of AL Rhoton, Jr).
RESECTION OF HYPOTHALAMIC HAMARTOMA
Preoperative lumbar puncture or placement of a lumbar drain affords brain relaxation, thus minimizing the need for brain retraction regardless of the approach. Intraoperative image guidance is a useful adjunct, especially for smaller lesions.
Please refer to the Supraorbital Craniotomy chapter for more details regarding the initial steps of the operation and exposure. The patient is positioned supine and the neck is slightly extended so that the frontal lobes are mobilized away from the skull base under the influence of gravity. A two-thirds bicoronal or soutar incision is performed; a pericranial flap is elevated, which may be used later if the frontal sinus is entered.
The eyebrow incision provides restricted access to the floor of the third ventricle due to the limited vertical reach of the craniotomy.

Figure 3: The patient is positioned supine with the head turned only 10 to 15 degrees away from the midline. The neck is extended slightly to allow the frontal lobes to fall away from the anterior skull base floor.
The surgeon performs a unilateral supraorbital craniotomy while avoiding the frontal sinus, if possible. As mentioned before, the craniotomy is contralateral to the laterality of the mass to allow a “cross-court” direct visualization of the lateral pole of the lesion. The dura is then incised in a “reverse-U” pattern and based anteriorly.
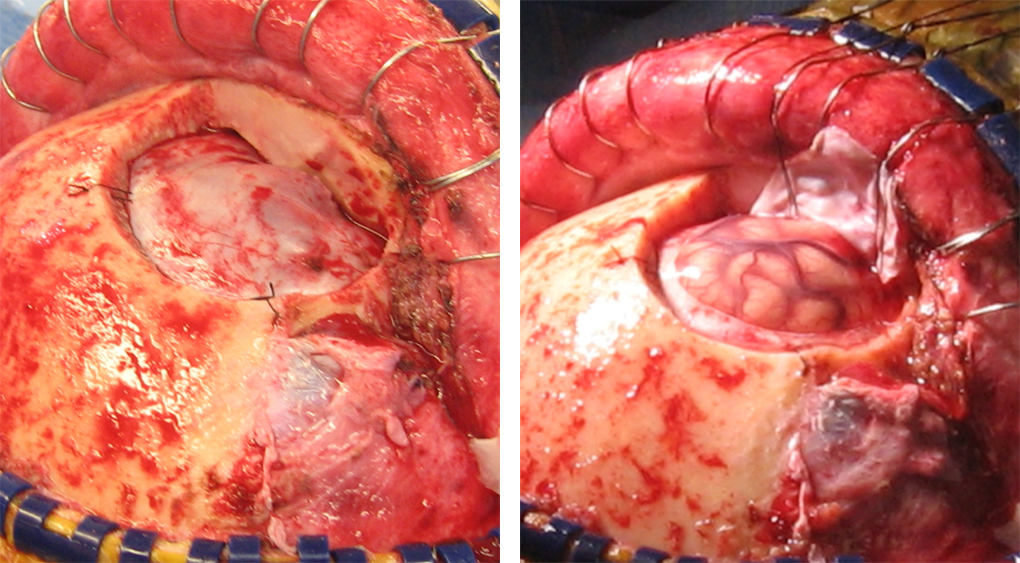
Figure 4: I do not remove the orbital rim for approaching a hypothalamic hamartoma because the operative trajectory is in the superior-to-inferior direction when I reach the third ventricular chamber.
INTRADURAL PROCEDURE
Cerebrospinal fluid (CSF) drainage via the lumbar drain facilitates brain mobilization before the opticocarotid cisterns are reached.

Figure 5: A right-sided supraorbital trajectory is shown. The inferior edge of the craniotomy is reduced to the level of the orbital roof. I use a piece of rubber glove (cut in the shape of a cotton patty) to slide the patty underneath the basal frontal lobe. Gentle elevation of the lobe exposes the ipsilateral optic nerve.

Figure 6: Continued gentle mobilization of the frontal lobe using dynamic retraction allows additional CSF release from the opticocarotid cisterns. The optic nerve is then followed posteriorly to the chiasm. The basal frontal lobe is released from the entire anterior optic apparatus and the anterior cerebral arteries are identified.
The lamina terminalis forms part of the anterior wall of the third ventricle and is attached to the superior optic chiasm. This relationship creates the optic recess within the third ventricle and the lamina terminalis recess in the suprachiasmatic space notable for its relationship to the A1 segment and the anterior communicating artery complex, as well as the key perforating arteries, including the recurrent artery of Huebner.
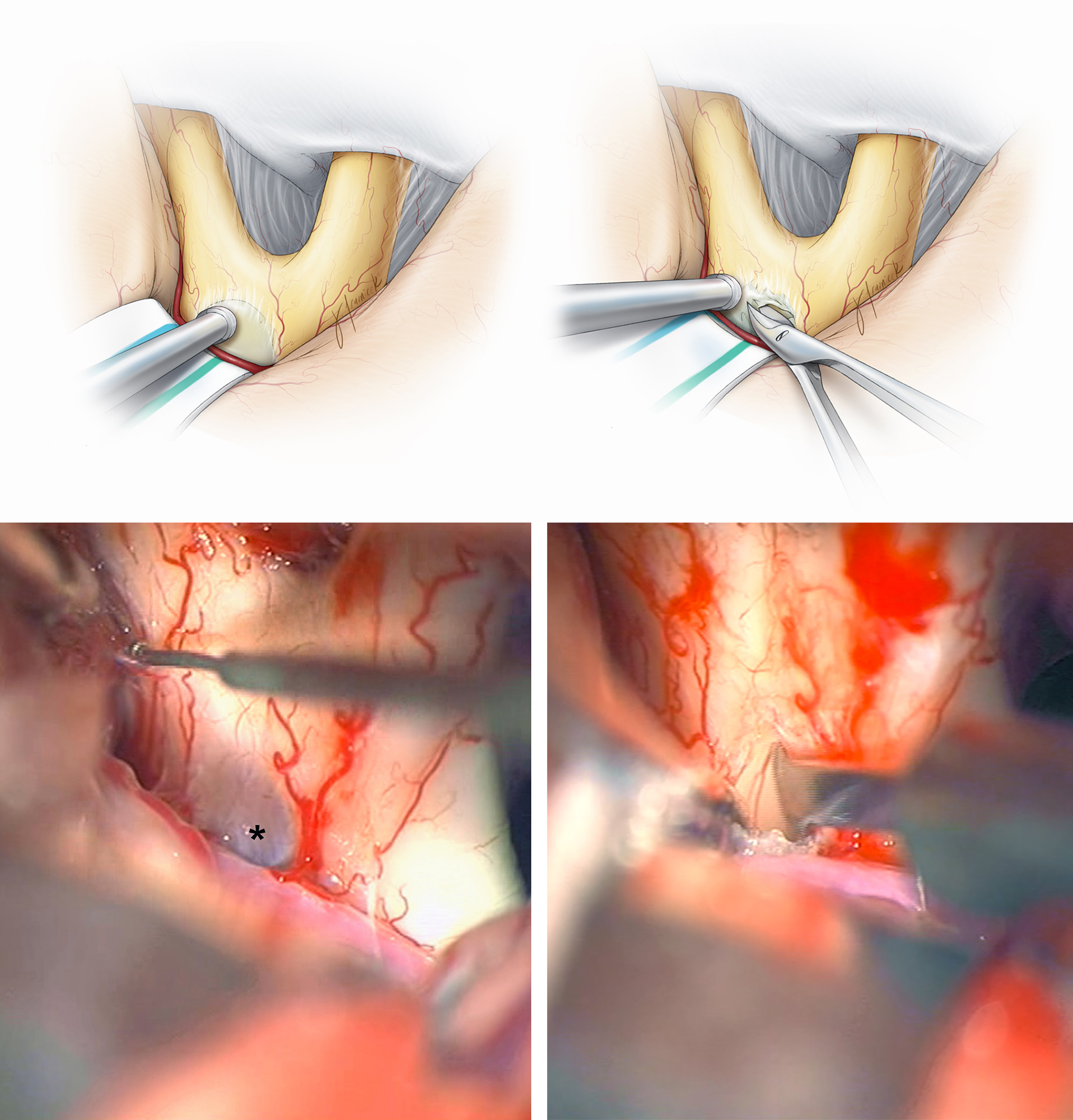
Figure 7: The exposure of the lamina terminalis and the anterior cerebral artery is shown (the images in the left column). The lamina is thin and relatively transparent, features that differentiate it from the rest of the chiasm. An incision in the lamina terminalis reveals the floor of the anterior third ventricle and the lesion (images of the right column). The perforating arteries arising from the anterior communicating artery complex and supplying the superior chiasm are preserved. Coagulation is kept to a minimum.

Figure 8: The working space is deep and dynamic retraction provides limited views of the operative target. I use an arachnoid knife to expand the initial crucial incision in the lamina terminalis. This instrument allows adequate visualization around its tip to avoid blind maneuvers that may lead to inadvertent injury to the surrounding vital structures. Next, the operative view is directed inferiorly toward the floor of the third ventricle. This superior-to-inferior trajectory around the lamina terminalis requires strategic dynamic mobilization of the frontal lobe to avoid subfrontal injury. The operative maneuvers must be conducted deliberately and efficiently without uninterrupted excessive retraction on the lobe. The dynamic force of the suction device exerts only periodic retraction on the subfrontal area during key maneuvers for removal of the mass.

Figure 9: Next, the rubbery and grayish hamartoma is slowly separated and carefully removed from the relatively normal walls of the hypothalamus using angled dissectors. The perilesional area is left behind and only the obviously abnormal tissue is disconnected. Pituitary rongeurs facilitate piecemeal evacuation of the mass. The borders of the mass are marked with blue arrows in the left lower photograph.

Figure 10: At the end of resection, the hamartoma-hypothalamic interface is left untouched. Aggressive resection is not advised.
Closure
Closure is conducted in standard fashion. If the frontal sinus was entered, it will be exenterated.
Postoperative Considerations
The patient is admitted postoperatively to the intensive care unit for continuous vital sign monitoring, blood pressure control, and hourly neurologic examinations. Frequent lab draws are obtained for close monitoring of the electrolyte and endocrine status. Postoperative MR imaging is usually obtained within the first 48 hours. Supratherapeutic levels of anticonvulsant medications are advised because the risk of perioperative seizures is significant.
Pearls and Pitfalls
- Hypothalamic hamartomas are exceedingly rare lesions associated with precocious puberty and seizures. Cognitive, psychiatric, and behavioral changes may also be present.
- Although gelastic-type seizures are the hallmark clinical finding with these lesions, they are not pathognomonic.
- Several surgical approaches to the anterior third ventricle are available, each with its own advantages and limitations.
- The subfrontal translamina terminalis approach provides a reasonable pathway for reaching the lesion and its radical subtotal removal. Aggressive resection is not attempted.
Contributors: Kashif Shaikh, MD, and Ian White, MD
References
Addas B, Sherman EM, Hader WJ. Surgical management of hypothalamic hamartomas in patients with gelastic epilepsy. Neurosurg Focus 2008;25:E8.
Amstutz DR, Coons SW, Kerrigan JF, et al. Hypothalamic hamartomas: correlation of MR imaging and spectroscopic findings with tumor glial content. Am J Neuroradiol 2006; 27:794–798.
Arita K, Kurisu K, Kiura Y, et al. Hypothalamic hamartoma. Neurol Med Chir (Tokyo) 2005;45:221–231.
Berkovic SF, Kuzniecky RI. Andermann F. Human epileptogenesis and hypothalamic hamartomas: new lessons from an experiment of nature. Epilepsia 1997;38:1–3.
Berkovic SF, Arzimanoglou A, Kuzniecky R, et al. Hypothalamic hamartoma and seizures: a treatable epileptic encephalopathy. Epilepsia 2003;44:969–973.
Cascino GD, Andermann F, Berkovic SF, et al. Gelastic seizures and hypothalamic hamartomas: evaluation of patients undergoing chronic intracranial EEG monitoring and outcome of surgical treatment. Neurology 1993;43:747–750.
Hahn FJ, Leibrock LG, Huseman CA, et al. The MR appearance of hypothalamic hamartoma. Neuroradiology 1988;30:65–68.
Harvey AS, Freeman JL, Berkovic SF, et al. Transcallosal resection of hypothalamic hamartomas in patients with intractable epilepsy. Epileptic Disord 2003;257–265.
Kulwin C, Chan D, Ting J, et al. Endoscopic endonasal transplanum transtuberculum resection of a large solid choroid plexus papilloma of the third ventricle. J Clin Neurosci 2014;21:1263–1266.
Jung H, Neumaier Probst E, Hauffa BP, et al. Association of morphological characteristics with precocious puberty and/or gelastic seizures in hypothalamic hamartoma. J Clin Endocrinol Metab 2003;88:4590–4595.
Jung H, Parent AS, Ojeda SR. Hypothalamic hamartoma: a paradigm/model for studying the onset of puberty. Endocr Dev 2005;8:81–93.
Kuzniecky R, Guthrie B, Mountz J, et al. Intrinsic epileptogenesis of hypothalamic hamartomas in gelastic epilepsy. Ann Neurol 1997;42:60–67.
Leal AJ, Passao V, Calado E, et al. Interictal spike EEG source analysis in hypothalamic hamartoma epilepsy. Clin Neurophysiol 2002;113:1961–1969.
Maixner W. Hypothalamic hamartomas--clinical, neuropathological and surgical aspects. Child Nerv Syst 2006;22:867–873.
Mullatti N. Hypothalamic hamartoma in adults. Epileptic Disord 2003;5:201–204.
Mullatti N, Selway R, Nashef L, et al. The clinical spectrum of epilepsy in children and adults with hypothalamic hamartoma. Epilepsia 2003;44, 1310–1319.
Munari C, Kahane P, Francione S, et al. Role of the hypothalamic hamartoma in the genesis of gelastic fits (a video-stereo-EEG study). Electroencephalogr Clin Neurophysiol 1995;95:154–160.
Savard G, Bhanji NH, Dubeau F, et al. Psychiatric aspects of patients with hypothalamic hamartoma and epilepsy. Epileptic Disord 2003;5:229–234.
Shim KW, Chang JH, Park YG, et al. Treatment modality for intractable epilepsy in hypothalamic hamartomatous lesions. Neurosurgery 2008;62:847–856; discussion 856.
Takeuchi J, Handa H, Miki Y, et al. Precocious puberty due to a hypothalamic hamartoma. Surg Neurol 1979;11:456–460.
Tassinari CA, Riguzzi P, Rizzi R. Gelastic seizures, in Tuxhorn I, Holthausen H, Boenighk K (eds): Pediatric Epilepsy Syndromes and Their Surgical Treatment. John Libbey, London, England; 1997:429–446
Weissenberger AA, Dell ML, Liow K, et al. Aggression and psychiatric comorbidity in children with hypothalamic hamartomas and their unaffected siblings. J Am Acad Child Adolesc Psychiatry 2001;40:696–703.
Related Materials
Available Through the Atlas
-

Neurosurgical treatment of hypothalamic hamartomas causing precoc...
-
Surgical strategies for approaching hypothalamic hamartomas causi...
-
Surgical approaches to hypothalamic hamartomas
-
Radiosurgery for hypothalamic hamartomas
-
Repeat surgery for hypothalamic hamartoma in refractory epilepsy
-
Combined open microsurgical and endoscopic resection of hypothala...
-
Hypothalamic hamartomas. part 2. surgical considerations and outc...
Unavailable Through the Atlas
-
Intrinsic epileptogenesis of hypothalamic hamartomas in gelastic...
-
Gelastic seizures and hypothalamic hamartomas: evaluation of pati...
-

Gamma knife surgery for epilepsy related to hypothalamic hamartom...
-
Transcallosal resection of hypothalamic hamartomas, with control...
-
Resection of the lesion in patients with hypothalamic hamartomas...
-
Generalized epilepsy in hypothalamic hamartoma: Evolution and pos...
-
Transcallosal resection of hypothalamic hamartoma for intractable...
-
Surgical treatment of intractable seizures due to hypothalamic ha...
-
Endoscopic resection of hypothalamic hamartomas for refractory sy...
-
Electrophysiological properties of human hypothalamic hamartomas
-
Hypothalamic hamartomas and gelastic Epilepsy: A spectroscopic st...
-
Treatment modality for intractable epilepsy in hypothalamic hamar...
-
Cognitive functioning before and after surgical resection for hyp...
Please login to post a comment.